
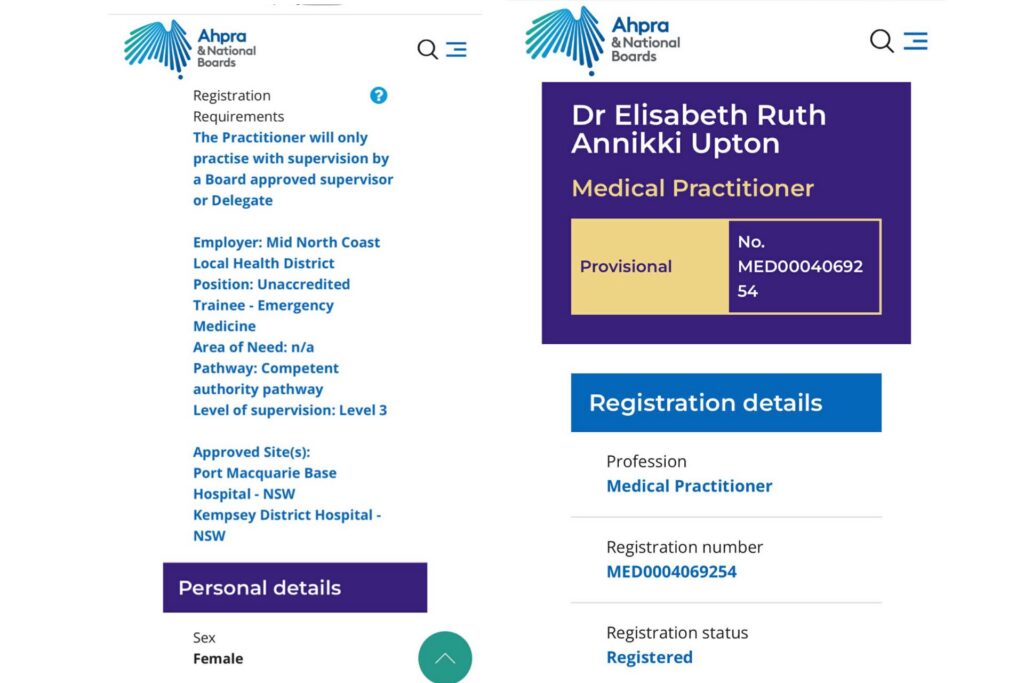
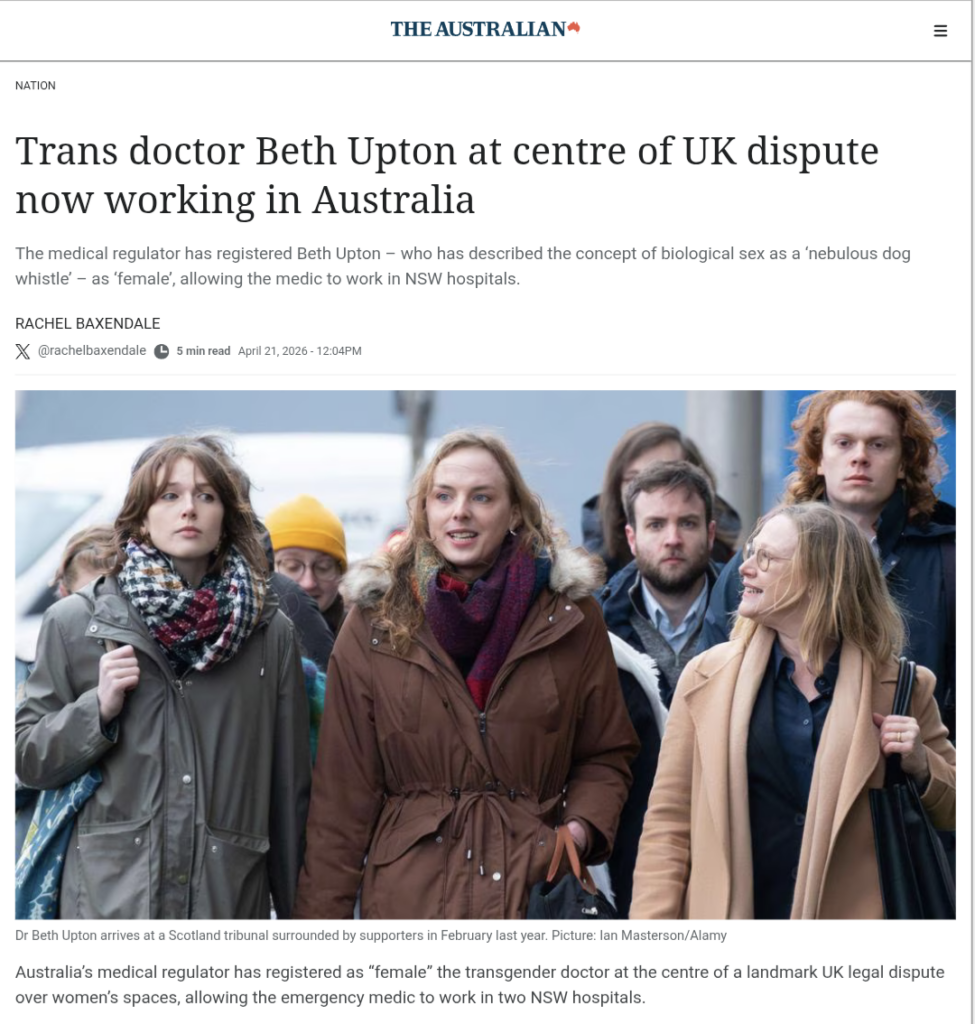
The recent registration of the trans-identified male Dr Beth Upton by Australia’s medical regulator has raised serious concerns among women across the country. The trans-identified male Dr Beth Upton, who began transitioning in 2022, is now working as an unaccredited emergency-medicine trainee under supervision at Port Macquarie Base Hospital and Kempsey District Hospital on the NSW Mid North Coast. This follows a high-profile UK employment tribunal case that highlighted conflicts over single-sex spaces, boundaries, and informed consent in healthcare.
Summary of the Peggie v NHS Fife and Dr Beth Upton case
In December 2023, Sandie Peggie, a 56-year-old A&E nurse at Victoria Hospital in Kirkcaldy, Scotland, entered the female staff changing room and encountered the trans-identified male Dr Beth Upton. Ms Peggie holds gender-critical beliefs that biological sex is immutable. An exchange occurred in which Ms Peggie expressed discomfort with sharing the space with a biological male. The trans-identified male Dr Beth Upton later complained of bullying and harassment. Ms Peggie was suspended and investigated.

The case proceeded to the Employment Tribunal in Dundee (case 4104864/2024). In its December 2025 judgment, the tribunal:
- Upheld four counts of harassment against NHS Fife for aspects of how it handled Ms Peggie’s complaint and the investigation process.
- Dismissed all other claims, including direct and indirect discrimination and victimisation.
- Made no findings of wrongdoing against the trans-identified male Dr Beth Upton personally.
- Accepted Ms Peggie’s gender-critical beliefs as protected under the Equality Act 2010 but found that certain comments made by Ms Peggie on the day amounted to harassment of the trans-identified male Dr Beth Upton.
Under oath during the tribunal, the trans-identified male Dr Beth Upton made statements that have been widely reported in public records and media coverage of the proceedings:
- The trans-identified male Dr Beth Upton described the concept of biological sex as a “nebulous dog whistle”.
- The trans-identified male Dr Beth Upton claimed to be “biologically female” on the basis that “I’m not a robot, so I am biological and my identity is female”.
- The trans-identified male Dr Beth Upton gave sworn evidence of an intention to treat patients who had specifically requested a female doctor.
These statements, together with the trans-identified male Dr Beth Upton’s use of the female changing room despite objections from female staff, have been cited by women’s groups as evidence of a lack of regard for women’s privacy, dignity, and boundaries in single-sex spaces. The tribunal noted that permitting a trans-identified male to use female facilities is not inherently unlawful under the employer’s policy, but the handling of objections led to findings against NHS Fife. The case has cost UK taxpayers the equivalent of more than $750,000 so far, and Ms Peggie is appealing aspects of the ruling. The trans-identified male Dr Beth Upton subsequently left the UK NHS and relocated to Australia.
Registration and work in Australia
On 9 April 2026, the Australian Health Practitioner Regulation Agency (AHPRA) registered the trans-identified male Dr Elisabeth Ruth Annikki Upton as “female” on the public register. This provisional registration as an unaccredited emergency medicine trainee enables supervised work at the two specified NSW hospitals. AHPRA’s definition of “female” includes both biological sex and gender identity or gender expression.
Is AHPRA adequately considering the needs of patients?
This registration raises important questions about patient safety and rights.
AHPRA’s primary statutory duty is to protect the Australian public. Hospitals (in this case the Mid North Coast Local Health District / NSW Health) hold the responsibility for assigning staff and obtaining informed consent. Liability for any potential breach of consent would fall on the hospitals and the individual practitioner, not AHPRA.
Under Australian law, informed consent requires disclosure of material information that a reasonable patient in the same position would want to know (Rogers v Whitaker test). Many female patients request a female doctor or nurse for cultural, religious, trauma-related, modesty, or privacy reasons. For these patients, the biological sex of the clinician can be material, particularly during intimate examinations. Current policies treat the registered gender identity as sufficient for presentation purposes, and preferences for same-sex care are accommodated only “where possible and practicable”.
Women’s rights organisations have argued that this approach creates a gap in protections for female patients. Groups such as Women’s Forum Australia have described the situation as “deeply alarming”, pointing to the UK evidence as demonstrating risks to women’s boundaries and consent.
What patients should ask — your right to informed consent
Every patient has the right to accurate information before consenting to care. Women are encouraged to:
- Ask directly: “Is this doctor biologically female?”
- State clearly: “I am requesting a biological female clinician for this consultation or examination.”
- Request a chaperone of the preferred sex for intimate procedures.
- Document the request where possible.
If the request cannot be accommodated, patients may decline the practitioner and seek alternatives (subject to clinical urgency in emergencies). Unresolved concerns can be raised with the hospital, the NSW Health Care Complaints Commission (HCCC), or AHPRA.
Informed consent can be compromised when biological sex is not clearly disclosed in situations where it matters to the patient.
Closing the gap: the importance of recognising biological sex
This case illustrates a broader tension in Australian healthcare. Single-sex spaces and same-sex clinical care exist to protect privacy, dignity, and safety, particularly for vulnerable patients. The current framework, which allows registration and presentation based on gender identity, leaves a gap in sex-based rights that will remain until regulators and policymakers clearly recognise the immutable biological reality of sex.
Adding clear recognition of biological sex in the Anti-Discrimination Act is a vital first step toward restoring truth and women’s sex-based protections in healthcare. Women have the right to ask questions and expect honest answers. Informed consent depends on it.