
The second day of the inaugural Coalition Advancing Scientific Care (CASC) Gender Healthcare Summit began early, with a warm welcome from CASC President, Dr Patrick Clarke. His opening remarks set the tone for a day filled with evidence, ethics, and courage.

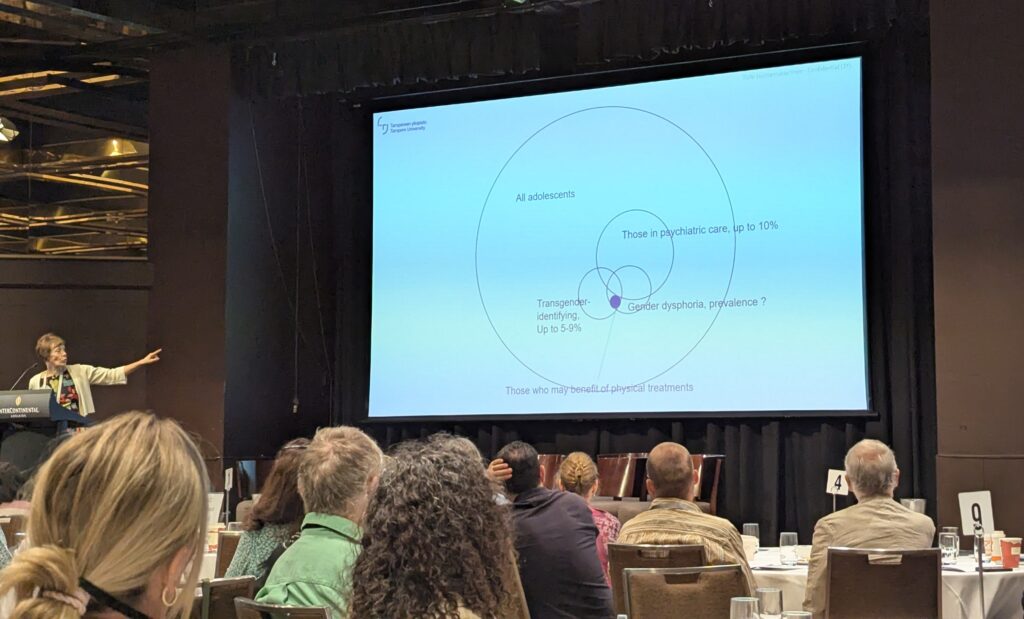
The first keynote came from Professor Riittakerttu Kaltiala, a leading adolescent psychiatrist from Tampere University, Finland. Her talk, “Mental Disorders Among Adolescents Presenting with Gender Dysphoria: Implications for Treatment,” offered a deeply insightful look at Finland’s journey in gender medicine.
Professor Kaltiala described how Finnish clinicians initially followed the Dutch protocol, but soon realised their patients did not match the patterns described in early studies—most were girls, and outcomes were not improving. “Adolescents with psychological issues continued presenting problems even after one year of cross-sex hormones,” she said. Concerned by these results, Finland began conducting its own studies.
Her conclusion was clear:
“You can modify the body, but the benefits for mental health have not been shown.”
Finland ultimately shifted to a more cautious model of care, prioritising psychotherapy and mental health over immediate affirmation—a model guided by evidence, not ideology.
Next up was Dr Helen Joyce, author of “Trans: When Ideology Meets Reality.” Her talk, “Gender Medicine Isn’t Science—It Isn’t Even Medicine,” was both sharp and illuminating. She argued that gender medicine lacks a coherent medical foundation, asking, “What does it mean to have a healthy gender?” She drew on Harriet Hall’s concept of “Tooth Fairy Science,” explaining, “At the end, you’ve deceived yourself into researching something that doesn’t exist.”

A highlight of the morning was the presentation of the Inaugural CASC Award to Professor Dianna Kenny, an Australian psychologist honoured for her courageous work supporting young people with gender dysphoria and their families.
Professor Kenny has faced relentless hostility for challenging the medicalised “gender-affirming” model in Australia—smears, threats, and professional complaints designed to silence her. In her acceptance speech, she said:
“The award provides a welcome counterpoint to the endless abuse I’ve received from trans activists and, worse, the persecution from my own profession.
I’ve been called a transphobe, a fascist, a conversion therapist, and even a danger to society. The morning after the launch of my book inTRANSigence, someone in France posted that I should be killed.”
Despite the harassment, she remains resolute:
“I need to create more necessary trouble to help redeem the soul of Australia. The stakes are high for a generation of our young people—and losing is not an option.”

Following this moving moment, Dr Roberto D’Angelo delivered an excellent talk titled “Why Psychotherapy Is Not Conversion Therapy.” He explained that genuine psychotherapy supports the autonomy of gender-distressed youth through open, curious exploration—not predetermined outcomes.
“There’s no way for clinicians to know who will benefit from transition and who won’t,” he noted. True informed consent, he reminded us, requires time, understanding, and honesty.
After lunch, Dr Alison Clayton presented “Evidence for Social Transition.” She reviewed studies showing that evidence supporting social transition as a mental health intervention is weak—and that, in some cases, early social transition may actually worsen outcomes. She warned:
“Given that most children with gender-related distress grow up to be homosexual rather than transgender adults, early social transition could act as a form of conversion therapy for some children.”

Next, Dr Dylan Wilson spoke on “Hormones, Puberty and Children: The Illogicality of Treatments in Gender Clinics.” He reminded the audience that puberty is a crucial developmental phase:
“This is the only situation in medicine where it’s considered acceptable to deliberately push a child’s hormones far outside the normal range.”
Dr Patrick Clarke, in his presentation “The Suicide Myth,” tackled one of the most pervasive misconceptions in this field:
“There is no evidence that interventions such as puberty blockers, cross-sex hormones, or surgery reduce suicide rates among adolescents with gender dysphoria. In fact, some evidence suggests the opposite.”
The day continued with Barrister Belle Lane, who joined remotely to discuss the legal landscape of gender-related cases in Australia. She reviewed key cases—Re Jamie (2013), Re Kelvin (2017), and Re Devin (2025)—explaining how the courts have grappled with questions of parental consent, Gillick competence, and the lack of scientific evidence underpinning gender treatments for minors. The Re Devin case, she noted, was significant because Justice Strum scrutinised the evidence presented by gender clinics and found it lacking in scientific rigour.
The afternoon concluded with a lively Q&A panel featuring Dr Andrew Amos and others, exploring how Australia can restore evidence-based practice and protect children from ideology-driven care.

As the summit drew to a close, there was a shared sense of optimism among attendees—a feeling that real progress is being made. It was an inspiring and thought-provoking event, filled with evidence, courage, and collaboration, all focused on restoring integrity to gender healthcare and protecting the wellbeing of children.
The path ahead won’t be simple, but with persistence and courage, change is already underway.

The inaugural Gender Healthcare Summit was organised by the Coalition Advancing Scientific Care (CASC). An inspiring beginning to what will surely become a landmark event in the movement for evidence-based, ethical healthcare.
