
The recently released WPATH Files expose disturbing internal communications among clinicians responsible for the so-called “Standards of Care.” These exchanges show that WPATH is not a scientific or evidence-based organisation, but one driven by ideology and activism.
WPATH and the Repetition of Medical Scandals
History provides sobering lessons about what happens when ideology or medical enthusiasm overtakes scientific evidence and patient safeguarding. The WPATH files reveal a dangerous parallel: just as lobotomies, thalidomide, and DES once harmed thousands under the banner of “progress,” the gender-affirming care model risks repeating these same mistakes with vulnerable children and adolescents.
Lessons From Past Medical Scandals
- Lobotomies: Once hailed as a revolutionary cure for mental illness, lobotomies were carried out on thousands — even children — despite little evidence of benefit. The procedure left countless people disabled, a warning of how medical fads can override patient welfare.
- Thalidomide: Marketed in the 1950s as a safe drug for pregnant women, thalidomide caused catastrophic birth defects. The tragedy showed the cost of pushing untested treatments into mainstream use.
- DES (Diethylstilbestrol): Prescribed to prevent miscarriage, DES was later found to cause rare cancers and reproductive issues in the children of women who took it.
- Other psychiatric abuses: Forced sterilisation, chemical castration, and shock therapy were once accepted “treatments,” later condemned as unethical and harmful.
These scandals share a common thread: authority figures convinced themselves and the public that harmful interventions were safe and necessary — until the evidence proved otherwise.
WPATH Files: History Repeating Itself
The leaked internal conversations from WPATH expose a similar disregard for scientific evidence and child safety:
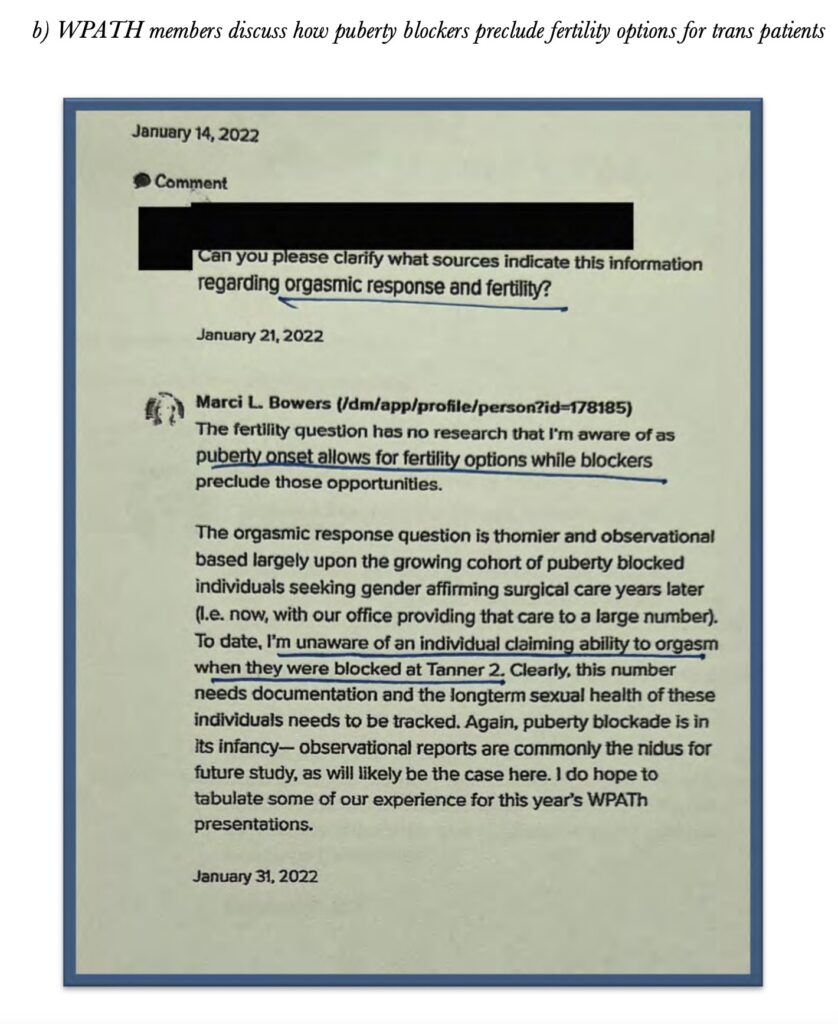
- Admitting lack of evidence: In private, WPATH members concede that the evidence base for puberty blockers, cross-sex hormones, and surgeries in youth is weak, incomplete, or absent — yet they still recommend these interventions as standard care.
- Children as young as 10 on hormones: Emails show clinicians discussing prescribing cross-sex hormones to children barely entering puberty, with little consideration for long-term effects.
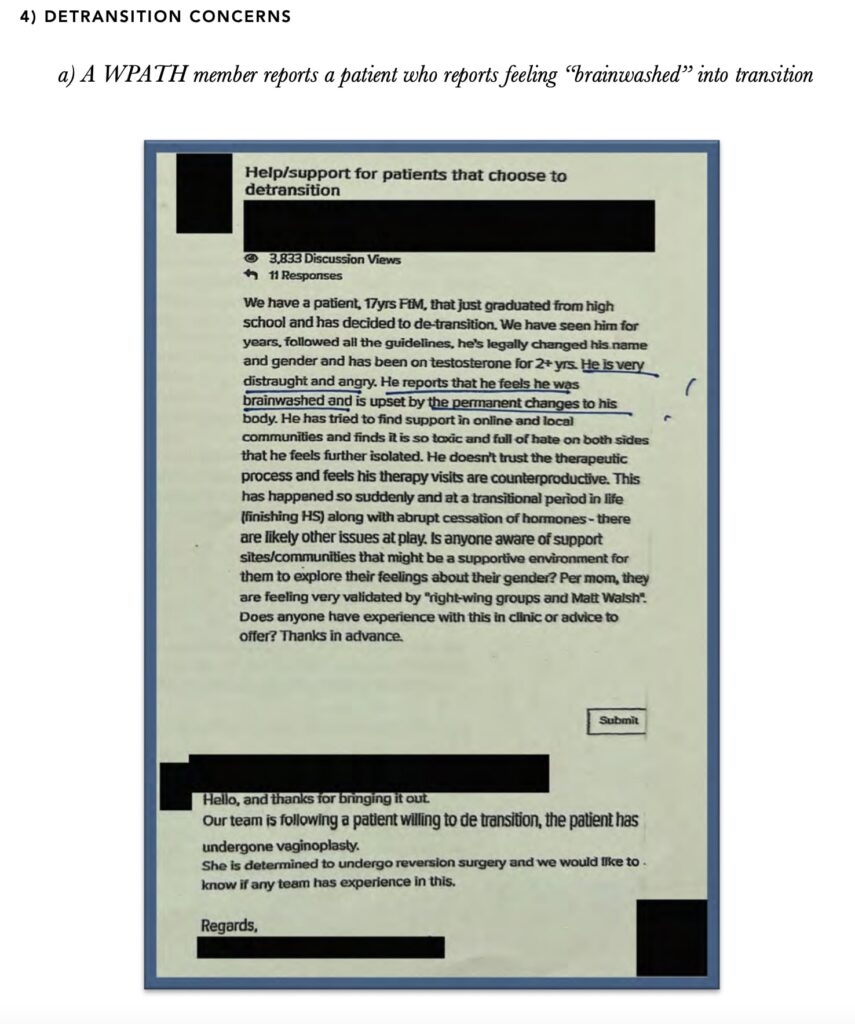
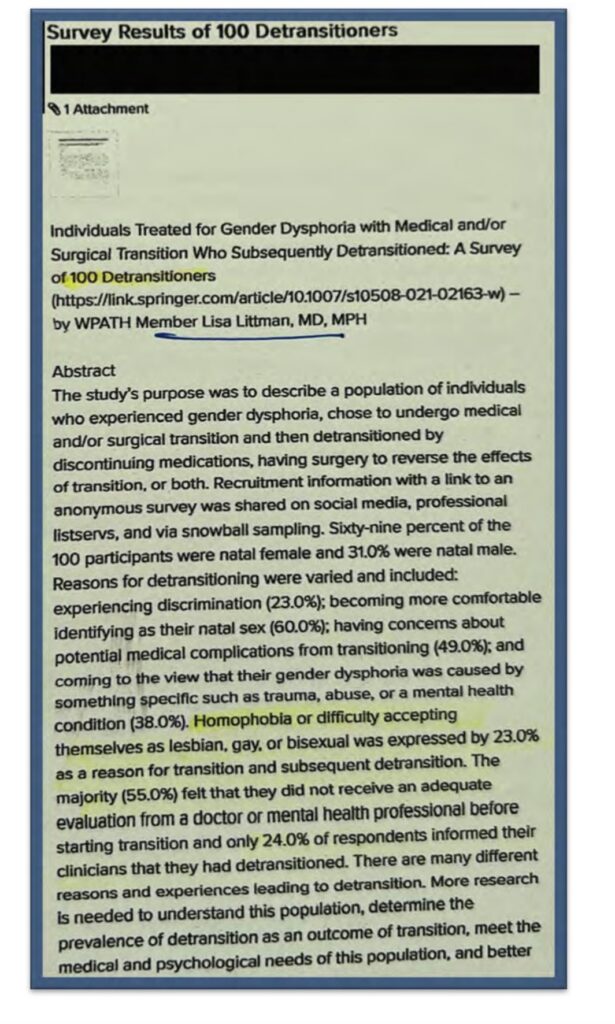
- Concerns about regret ignored: Some clinicians privately raise alarm about cases of detransition and lifelong medical harm, but these are brushed aside to preserve the “affirmation” model.
- Parental exclusion: Internal discussions acknowledge that parents are often sidelined, with clinicians deliberately framing resistance as “unsafe parenting” rather than engaging with legitimate concerns.
One striking example shows clinicians debating how to justify including “eunuch” identity in the WPATH manual. Rather than questioning whether such categories are medically appropriate, they rationalise how to defend them — exposing that ideology, not science, drives decisions.
Examples from the Emails & Conversations
- On prescribing puberty blockers without evidence
- On surgeries in minors

- On lack of evidence for gender identity as a concept
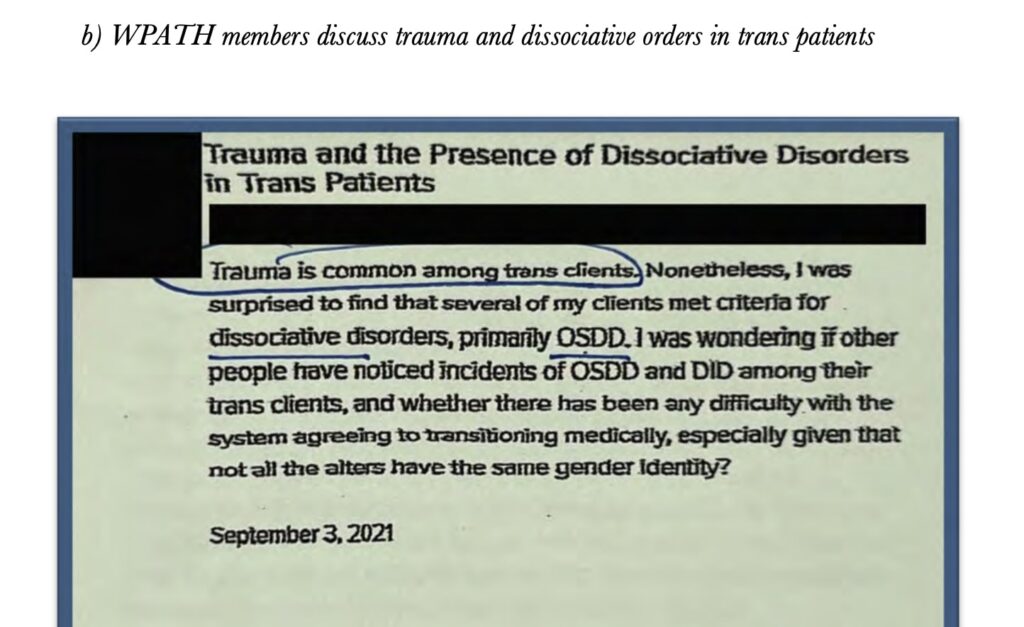
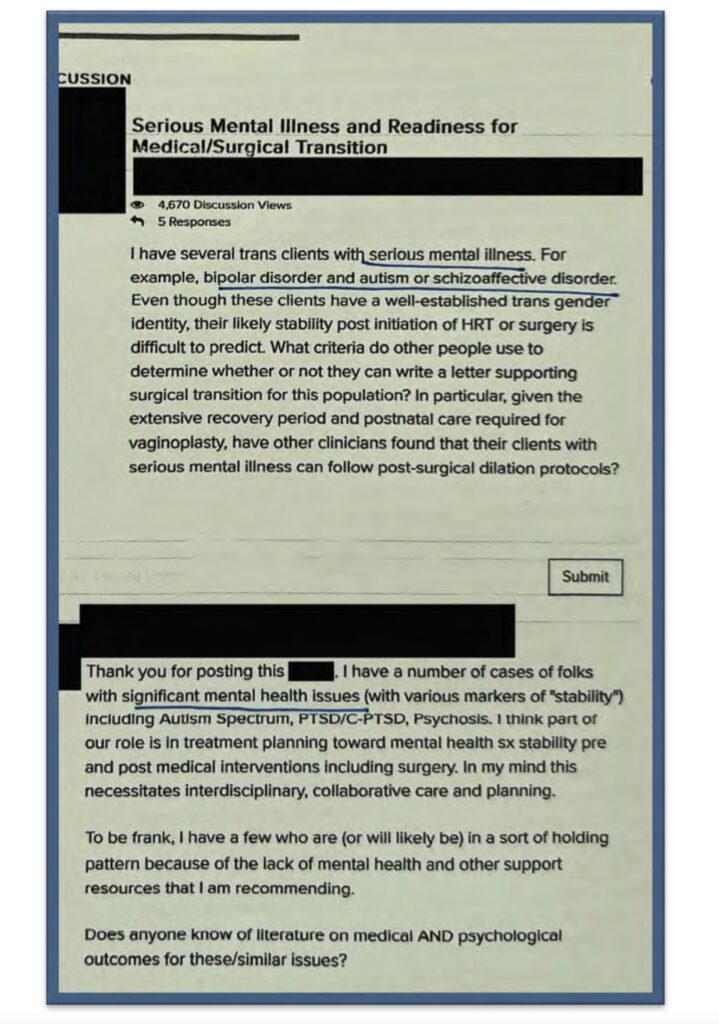
- On patient regret and lack of safeguards
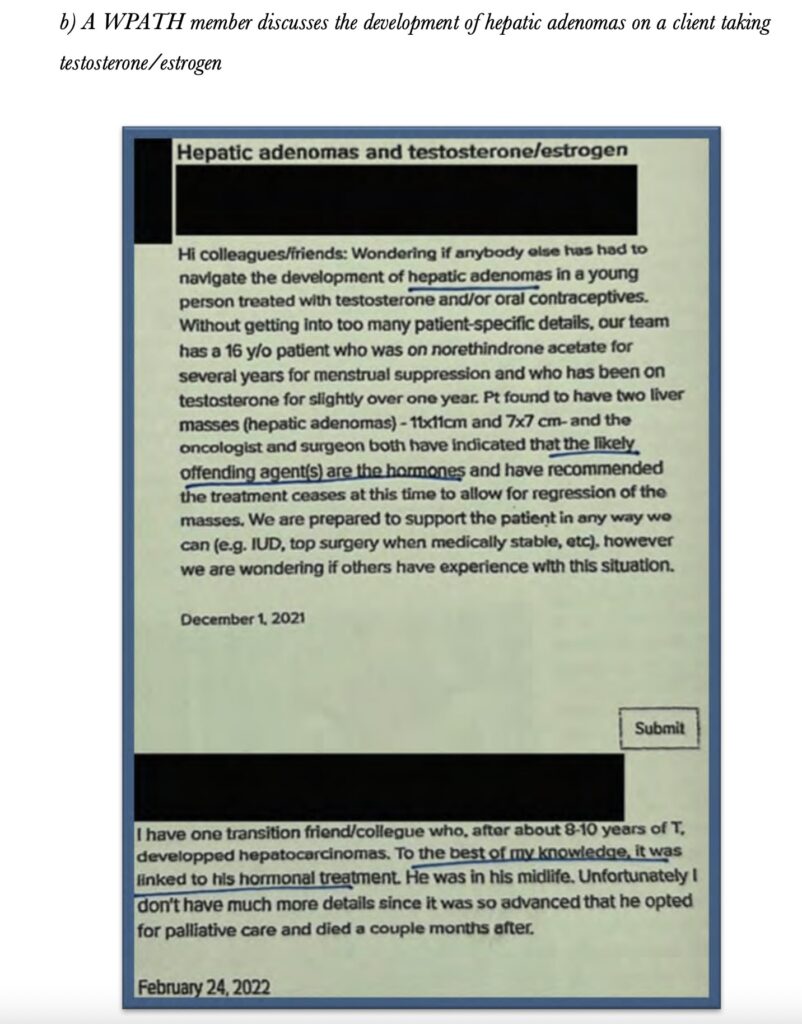
- On patients suffering from complications
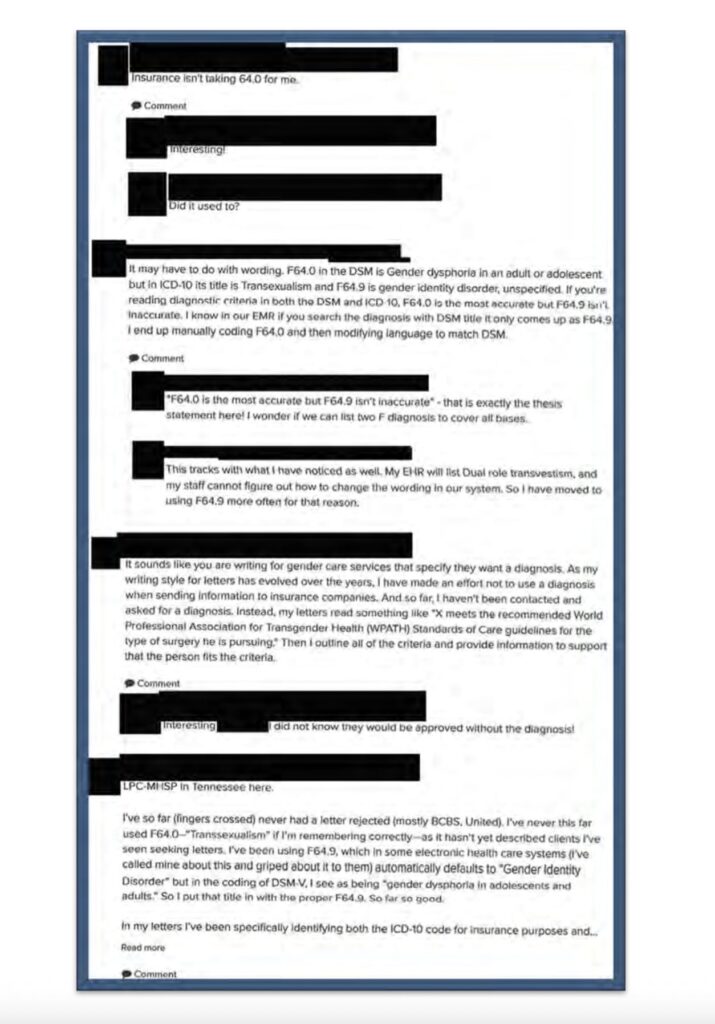
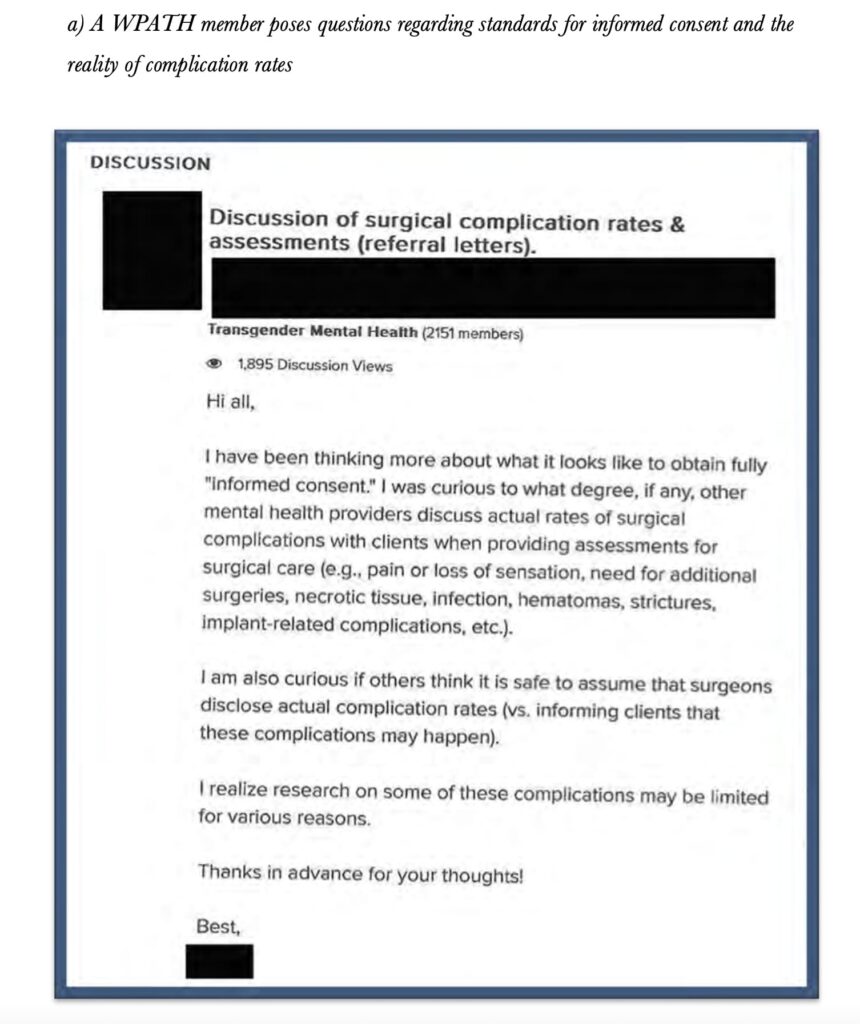
6. On difficulty of reach full informed consent
Then and Now: The Same Pattern
The parallel is unmistakable. Just as lobotomies and DES were introduced without rigorous study and inflicted lifelong harm, WPATH today promotes gender-affirming care — an ideology-driven model that:
- Lacks a solid evidence base (as their own emails admit).
- Treats children as experimental subjects.
- Overrides parental rights and child safeguarding laws.
- Ignores mounting evidence of harm, including cases of sterility, loss of sexual function, and regret.
Future generations may look back on this moment the way we now look back on lobotomies or thalidomide: as a catastrophic medical scandal, enabled by professionals who abandoned evidence for ideology.